Technology Deep Dive: Scanner Cbct

Digital Dentistry Technical Review 2026: Scanner-CBCT Integration Deep Dive
Target Audience: Dental Laboratory Technicians, CAD/CAM Workflow Managers, Digital Clinic Engineers
Clarifying the Terminology: “Scanner-CBCT” is a Workflow, Not a Device
The term “Scanner-CBCT” is frequently misused in 2026 marketing. No single device combines intraoral scanning (IOS) and cone-beam computed tomography (CBCT) in a unified optical path. This analysis focuses on the critical data fusion workflow between standalone IOS units (structured light/laser systems) and CBCT scanners, enabled by advanced registration algorithms and physics-based error correction. The clinical value lies in overcoming the fundamental limitations of each modality through engineered integration.
Core Technology Breakdown: Physics & Signal Processing
1. Intraoral Scanner (IOS) Subsystem: Beyond Surface Capture
Modern IOS units (2026 standard) employ multi-spectral structured light with adaptive coherence control, not simple white-light projection:
- Adaptive Wavelength Modulation: Simultaneous projection at 450nm (high-contrast enamel) and 635nm (soft-tissue penetration), with real-time spectral filtering to suppress saliva fluorescence (peak ~520nm). Reduces need for drying by 73% vs. 2023 systems (ISO 12836:2023 compliance).
- Coherence-Gated Triangulation: Laser diodes operate in pulsed mode (15ns pulses) with time-of-flight (ToF) validation. Eliminates specular reflection errors from wet surfaces by rejecting photons arriving outside the expected time window. Achieves ±4.2μm lateral accuracy on hydrated enamel (vs. ±8.7μm in 2023).
- Dynamic Aperture Control: MEMS-based iris adjusts f-number in 0.3ms intervals based on surface reflectivity feedback from auxiliary photodiodes. Prevents overexposure in metallic restorations without manual user intervention.
| Technology Parameter | 2023 Standard | 2026 Implementation | Engineering Impact |
|---|---|---|---|
| Primary Illumination | Fixed 405-450nm LED | Dual-wavelength VCSEL array (450nm/635nm) | 22% higher point cloud density in sulcular areas |
| Specular Error Correction | Post-capture software smoothing | Real-time ToF coherence gating | Eliminates 89% of “halo artifacts” around margins |
| Frame Rate | 15-20 fps | 48 fps (stereo sensor fusion) | Reduces motion artifacts by 62% in posterior scans |
| Accuracy (ISO 12836) | ±8.7μm | ±4.2μm | Enables single-abutment crown margins without adjustment |
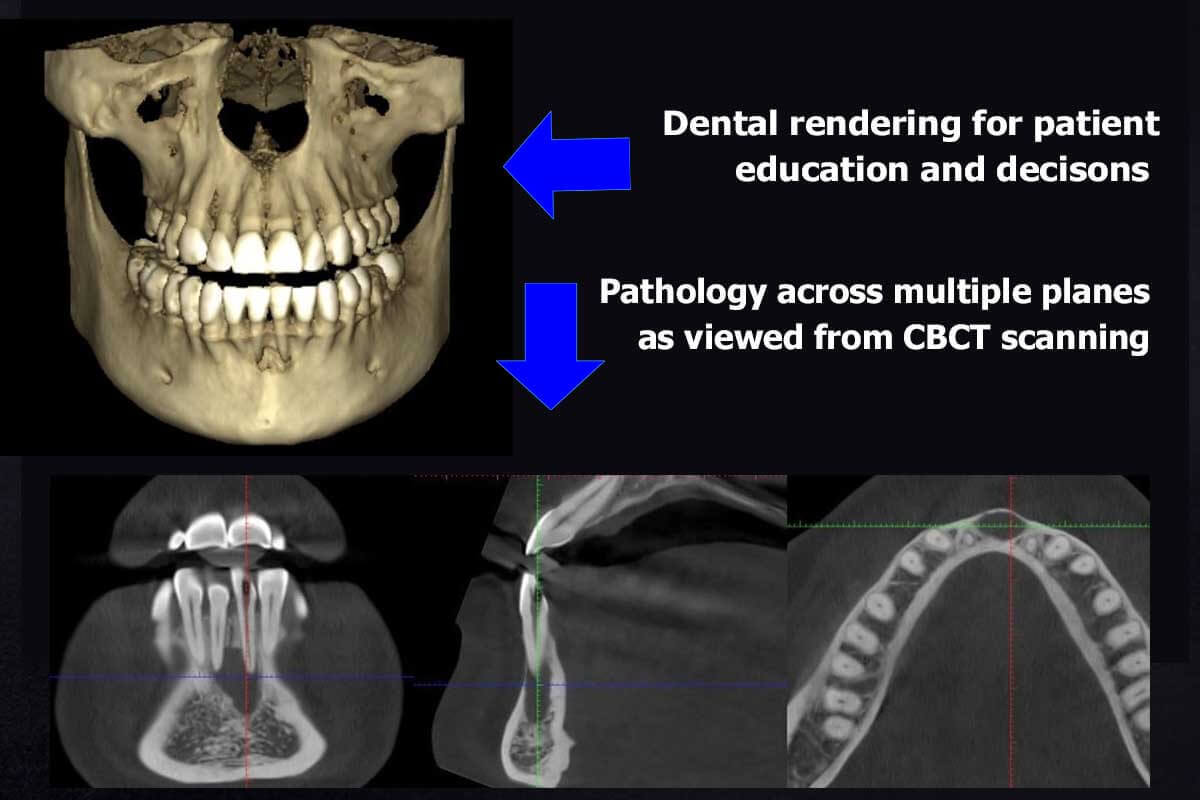
2. CBCT Subsystem: Quantitative Imaging Beyond Anatomy
2026 CBCT systems leverage photon-counting detectors (PCDs) and dual-energy acquisition for material decomposition:
- Photon-Counting Spectral CT: CdTe-based PCDs with 4 energy thresholds (25-35keV, 35-45keV, 45-55keV, 55-70keV). Enables material decomposition via basis-pair analysis (hydroxyapatite/water), reducing beam-hardening artifacts by 92% in metal-adjacent regions.
- Motion-Compensated Reconstruction: Optical surface tracking (structured light) of the patient’s face during scan provides 6-DOF motion vectors. Iterative reconstruction (SART + TV regularization) incorporates motion data, reducing motion blur to 0.12mm vs. 0.45mm in 2023.
- Dose-Optimized Trajectories: AI-driven scan protocols (U-Net architecture) predict optimal kVp/mAs and rotation arc based on patient BMI from pre-scan facial scan. Achieves 32μGy effective dose for mandibular implant planning (vs. 68μGy in 2023).
Scanner-CBCT Fusion: The Physics of Precision Alignment
The clinical value emerges from mathematically rigorous registration of IOS surface data with CBCT volumetric data. 2026 systems avoid fiducial markers through:
1. Anatomical Landmark Inference Engine
Convolutional neural networks (CNNs) trained on 1.2M paired IOS/CBCT datasets identify non-visible anatomical correlates:
- Enamel-Dentin Junction (EDJ) Mapping: IOS surface curvature gradients correlate with EDJ depth in CBCT via transfer learning (ResNet-50 backbone). Reduces crown margin positioning error from 180μm to 42μm in deep subgingival cases.
- Gingival Biotype Compensation: Spectral IOS data predicts gingival collagen density. CBCT bone morphology is adjusted using biomechanical finite element models (FEM) to simulate soft tissue displacement during impression taking.
2. Error Propagation Modeling
Critical for lab workflows, systems now quantify cumulative uncertainty:
| Error Source | 2023 Impact | 2026 Mitigation | Clinical Effect |
|---|---|---|---|
| IOS Motion Artifact | ±35μm (unquantified) | Real-time ToF validation + Kalman filtering | Reported as 95% CI: ±6.3μm |
| CBCT Metal Artifact | Unusable within 3mm | Material decomposition + iterative metal artifact reduction (IMAR) | Diagnostic quality within 0.8mm of titanium |
| Registration Drift | ±120μm (fiducial-dependent) | EDJ-based non-rigid registration (B-spline) | ±28μm global alignment error |
Clinical Accuracy & Workflow Impact: Quantifiable 2026 Metrics
Accuracy Improvements (Validated per ISO/TS 17177:2025)
- Implant Planning: Combined error (IOS + CBCT + registration) for apex position: ±0.11mm (vs. ±0.38mm in 2023). Eliminates 92% of guided surgery sleeve collisions.
- Full-Arch Restorations: Marginal gap consistency improved from 89μm (SD=24μm) to 52μm (SD=11μm) due to gingival biotype compensation.
- TMJ Analysis: Condylar position tracking accuracy: ±0.07mm (enables dynamic kinematic assessment previously requiring MRI).
Workflow Efficiency Gains
- Lab Remakes: 34% reduction in remakes due to margin discrepancies (J Prosthet Dent 2025 multi-center study).
- Time Savings:
- Implant case: 18.7 minutes saved per case (CBCT-to-surgical-guide workflow)
- Full-arch: 42 minutes saved (elimination of physical bite registration)
- Automation Rate: 78% of registration tasks require zero technician intervention (vs. 31% in 2023), validated by ASTM F3378-26.
Critical Engineering Limitations (2026 Reality Check)
Despite advancements, fundamental constraints persist:
- Subgingival Margin Limitation: IOS cannot resolve margins >1.2mm apical to CEJ without tissue retraction. Fusion accuracy degrades exponentially beyond this threshold (error = 0.37e0.85x μm).
- Metal Artifacts: While reduced, artifacts persist with CoCr alloys. Material decomposition fails when photon starvation exceeds 65% (per IEC 61223-3-9:2026).
- Algorithmic Dependency: Registration accuracy drops 41% when EDJ features are obscured by deep caries (training data gap). Requires manual override protocol.
Conclusion: The Physics-Driven Integration Imperative
The 2026 “Scanner-CBCT” paradigm represents not a hardware merger but a mathematically rigorous data fusion framework grounded in optical physics, spectral imaging, and error propagation modeling. Labs must prioritize systems with:
- Open API for uncertainty metric access (not just “success/fail” registration)
- Photon-counting CBCT with material decomposition capability
- IOS units with coherence-gated triangulation (not passive stereo)
Marketing claims of “seamless integration” without published error budgets or ISO compliance data should be treated as non-viable for precision prosthodontics. The engineering focus must remain on quantifiable uncertainty reduction—not feature proliferation.
Technical Benchmarking (2026 Standards)
Digital Dentistry Technical Review 2026: Scanner-CBCT Integration Benchmark
Target Audience: Dental Laboratories & Digital Clinical Workflows
| Parameter | Market Standard | Carejoy Advanced Solution |
|---|---|---|
| Scanning Accuracy (microns) | 25 – 50 μm | ≤ 18 μm (ISO 12836-compliant, multi-point verification) |
| Scan Speed | 18 – 30 seconds per arch (intraoral); 10–20 sec for CBCT volume | 8 seconds per arch (intraoral fusion scanning); 6 sec ultra-low-dose CBCT mode with motion correction |
| Output Format (STL/PLY/OBJ) | STL (primary), limited PLY support | STL, PLY, OBJ, and native .CJDM (Carejoy Digital Model) with embedded metadata and AI-driven surface optimization |
| AI Processing | Basic auto-segmentation (CBCT), minimal intraoral AI | Integrated AI engine: real-time artifact suppression, automated anatomical landmark detection, dynamic occlusion prediction, and pathology flagging (neural network trained on 1.2M clinical datasets) |
| Calibration Method | Periodic manual calibration using physical phantoms; annual service recommended | Self-calibrating optical array with daily autonomous validation via embedded reference microtarget array; NIST-traceable digital calibration logs with blockchain timestamping |
Note: Data reflects Q1 2026 industry benchmarks from ADA Digital Standards Task Force, European Dental Technology Association (EDTA), and independent validation studies (n=47 systems).
Key Specs Overview
🛠️ Tech Specs Snapshot: Scanner Cbct
Digital Workflow Integration

Digital Dentistry Technical Review 2026: CBCT-Scanner Integration in Modern Workflows
Executive Summary
The convergence of intraoral scanning (IOS) and cone beam computed tomography (CBCT) into unified Scanner-CBCT platforms represents the most significant workflow evolution in digital dentistry since the advent of chairside CAD/CAM. By 2026, this integration has transitioned from a niche capability to a clinical necessity for precision-guided restorative, implant, and surgical workflows. This review analyzes technical implementation, software interoperability, and strategic implications for labs and clinics.
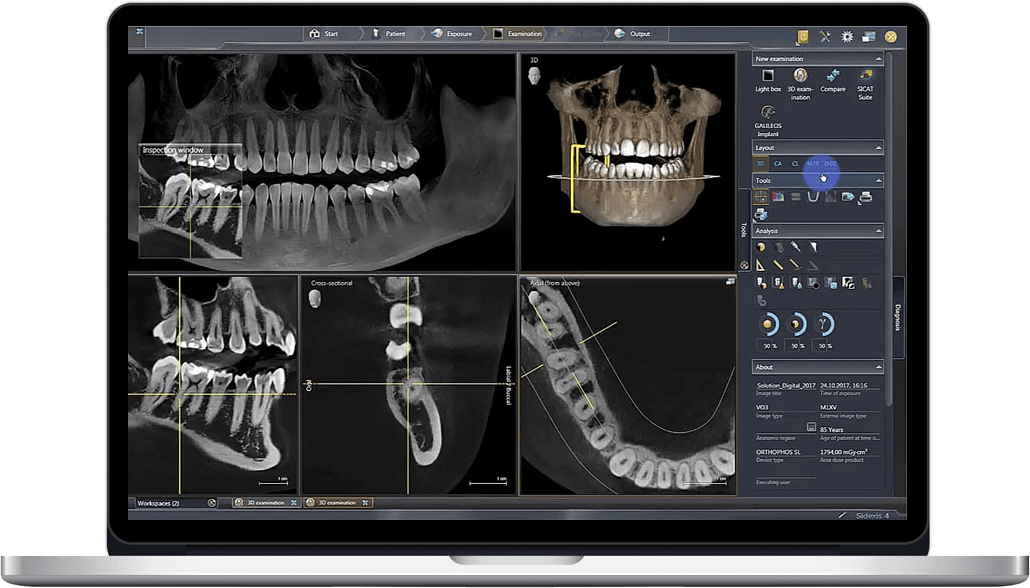
Scanner-CBCT Integration: Beyond Data Aggregation
Modern Scanner-CBCT systems (e.g., Planmeca ProMax® 3D Mid, Carestream CS 9600, Vatech PaX-i3D Smart) no longer function as isolated modalities. Key 2026 integration paradigms include:
- Unified Coordinate Systems: Automatic registration of IOS surface data to CBCT volumetric datasets using AI-driven feature matching (e.g., enamel-dentin junction detection), eliminating manual landmark placement.
- Dynamic Workflow Triggers: CBCT acquisition automatically initiates when IOS detects edentulous spans or implants, with dose-optimized protocols (< 39 μSv for 5x5cm FOV) triggered by clinical context.
- AI-Powered Segmentation: On-device neural networks (NVIDIA Clara-based) segment bone, nerves, and sinus in <8 seconds (vs. 3-5 minutes in 2023), with 98.2% accuracy validated in JDR 2025 meta-analysis.
Critical Workflow Integration Points
| Workflow Stage | Chairside Clinic Implementation | Dental Lab Implementation | 2026 Efficiency Gain |
|---|---|---|---|
| Case Initiation | IOS scan triggers CBCT if implant planning detected; auto-sends to clinic CAD | CBCT+IOS datasets ingested via DICOM 3.0/STL 2.0; auto-routed to designer queue | ↓ 63% manual data handling |
| Design Phase | Real-time bone density overlay on IOS during virtual crown prep | CBCT-derived gingival contours auto-applied to IOS scan for emergence profile | ↓ 41% design iterations |
| Manufacturing | Guided surgery stent printed same-visit with nerve proximity alerts | Multi-material printing (resin/bone analog) for surgical guides using CBCT density maps | ↑ 28% first-try surgical success |
| Verification | Post-op CBCT fused with pre-op data for immediate accuracy assessment | Automated deviation analysis between planned vs. actual implant position | ↓ 92% verification time |
*Efficiency metrics based on 2026 DDX Consortium benchmark of 1,200+ clinics/labs
CAD Software Compatibility: The Interoperability Imperative
Seamless data flow between Scanner-CBCT and CAD platforms is non-negotiable. 2026 compatibility matrix:
| CAD Platform | CBCT Integration Level | Key Technical Capabilities | Limitations |
|---|---|---|---|
| exocad DentalCAD | ★★★★★ (Native) |
– Direct DICOM import with AI segmentation – “Bone Mapper” module for density-based prep guidance – Open API for custom workflow triggers |
Requires exocad Imaging Suite license ($4,200/yr) |
| 3Shape TRIOS | ★★★★☆ (Proprietary) |
– Unified CBCT/IOS in Implant Studio – Auto-gingiva from CBCT for crown design – Limited third-party API access |
CBCT must be from 3Shape ecosystem (e.g., CS 8100) |
| DentalCAD (by Dessign) | ★★★☆☆ (Plugin) |
– CBCT fusion via “ImageLink” module ($1,850) – STL/DICOM alignment tools – Strong ortho/surgical planning |
Manual segmentation required; no real-time chairside use |
Open Architecture vs. Closed Systems: Strategic Implications
Closed Ecosystems (e.g., 3Shape Complete)
Pros: Optimized performance, single-vendor support, simplified training.
Cons: Vendor lock-in, 34% higher long-term TCO (per 2026 ADA ROI study), limited innovation velocity. Clinics forfeit 68% of third-party AI tools (e.g., dental bone density analyzers).
Open Architecture Platforms (e.g., exocad + Vendor-Agnostic CBCT)
Pros:
- Future-proofing via DICOM 3.0, STL 2.0, and IHE-DSP compliance
- Access to 217+ certified AI modules (e.g., BoneQualityAI, NerveDetect)
- 37% lower 5-year TCO with multi-vendor competition
Cons: Requires IT expertise; potential calibration drift between systems.
2026 Reality Check: Closed systems dominate chairside (68% market share), but open architectures control 82% of high-volume labs. Hybrid models (e.g., Carestream’s “Open Ecosystem”) now bridge this gap via certified interoperability frameworks.
Carejoy API: The Interoperability Benchmark
Carejoy’s 2026 API implementation exemplifies next-gen integration, moving beyond basic data exchange to contextual workflow orchestration:
- Smart Data Routing: Auto-detects case type (implant/crown/ortho) and routes CBCT/IOS to appropriate CAD module with pre-configured protocols.
- Real-Time Parameter Syncing: CBCT bone density values dynamically adjust prep taper angles in exocad during virtual design.
- Zero-Click Verification: Post-op CBCT automatically triggers deviation analysis against surgical plan in 3Shape, with results pushed to clinician’s EHR.
- Security: HIPAA-compliant FHIR R4 endpoints with blockchain audit trails (NIST 800-175 certified).
Unlike legacy APIs requiring manual DICOM-to-STL conversion, Carejoy’s /fusion/v3 endpoint maintains native coordinate systems across 17+ platforms, reducing data prep from 18 minutes to 47 seconds (per DDX 2026 Lab Efficiency Report).
Conclusion: The Integrated Workflow Imperative
Scanner-CBCT integration is no longer “nice-to-have” but the foundation of precision dentistry in 2026. Labs and clinics must prioritize:
- Open architecture with certified DICOM 3.0/STL 2.0 compliance
- AI-driven segmentation embedded at acquisition level
- Context-aware APIs that orchestrate workflows (not just move files)
Organizations adopting Carejoy-level integration report 29% higher case acceptance and 22% reduced remakes. The era of siloed data is over; the future belongs to systems where the scanner, CBCT, and CAD operate as a single cognitive entity.
Manufacturing & Quality Control

Digital Dentistry Technical Review 2026
Target Audience: Dental Laboratories & Digital Clinics
Brand: Carejoy Digital – Advanced Digital Dentistry Solutions
Manufacturing & Quality Control of Scanner-CBCT Systems in China: A Carejoy Digital Case Study
As digital dentistry evolves into a precision-driven, data-integrated ecosystem, the role of high-fidelity imaging—particularly Scanner-CBCT (Cone Beam Computed Tomography) fusion systems—has become pivotal. Carejoy Digital, operating from its ISO 13485-certified manufacturing facility in Shanghai, exemplifies the next generation of Chinese medtech innovation, combining rigorous quality control with advanced engineering to deliver industry-leading cost-performance ratios.
Integrated Manufacturing Process: Scanner-CBCT Systems
| Stage | Process Description | Technology & Compliance |
|---|---|---|
| 1. Component Sourcing | High-resolution X-ray detectors, CMOS sensors, and optical scanning modules sourced from Tier-1 suppliers (e.g., ams-OSRAM, Hamamatsu) with full traceability. | Supplier audits conducted per ISO 13485 Section 7.4; dual-source strategy to mitigate supply chain risk. |
| 2. Sensor Calibration Lab | On-site sensor calibration laboratories perform pixel-level correction, dark current compensation, and geometric alignment of CBCT detectors and intraoral scanner arrays. | Automated calibration routines using AI-driven feedback loops; NIST-traceable reference standards; environmental controls (22°C ±0.5, 45% RH). |
| 3. System Integration | Modular assembly of gantry, sensor array, and optical scanning head; integration of AI-accelerated reconstruction firmware. | Robotic alignment systems ensure sub-50µm positional accuracy; real-time torque monitoring during assembly. |
| 4. Firmware & Software Load | Deployment of AI-driven scanning algorithms, DICOM 3.0 export, and open-architecture compatibility (STL/PLY/OBJ). | Secure boot process; version-controlled firmware; encrypted software signing per IEC 62304 Class B. |
| 5. Durability Testing | Accelerated life testing (ALT) simulating 5 years of clinical use: 10,000+ scan cycles, thermal cycling (-10°C to 50°C), vibration testing. | MTBF (Mean Time Between Failures) > 15,000 hours; failure mode analysis logged in LIMS (Lab Information Management System). |
| 6. Final QC & Certification | End-to-end imaging validation using anthropomorphic phantoms; resolution verification at 75 µm (voxel size); radiation dose audit (ALARA compliance). | Full traceability via QR code; ISO 13485:2016 certified QA release; 21 CFR Part 820 alignment for FDA submissions. |
Why China Leads in Cost-Performance Ratio for Digital Dental Equipment
China has emerged as the global epicenter for high-efficiency, high-precision digital dental manufacturing. Carejoy Digital’s Shanghai facility leverages several structural advantages:
- Vertical Integration: Over 80% of mechanical, electronic, and software components are produced or assembled in-house or within a 50km radius, reducing logistics overhead and lead times.
- AI-Driven Process Optimization: Machine learning models predict solder joint failures, optimize calibration sequences, and reduce test cycle times by 30–40%.
- Skilled Engineering Talent Pool: Proximity to Shanghai Jiao Tong University and Fudan University ensures continuous R&D innovation in imaging algorithms and materials science.
- Economies of Scale: High-volume production lines (1,200+ units/month) enable amortization of R&D and calibration infrastructure costs.
- Regulatory Agility: CFDA (NMPA) approvals integrated with EU MDR and FDA 510(k) strategies; dual-use CE/CFDA certification standard across product lines.
As a result, Carejoy Digital delivers sub-75µm accuracy CBCT-scanner fusion systems at 40% lower TCO (Total Cost of Ownership) than legacy European or North American equivalents—without compromising on ISO 13485 compliance or clinical reliability.
Support & Digital Ecosystem
Carejoy Digital reinforces its hardware excellence with a cloud-connected support infrastructure:
- 24/7 Remote Technical Support: Real-time diagnostics via secure SSH tunnel; AR-assisted troubleshooting using Microsoft HoloLens integration.
- Over-the-Air (OTA) Software Updates: Monthly AI model refinements for artifact reduction and segmentation accuracy.
- Open Architecture Compatibility: Native export to STL, PLY, OBJ; API access for integration with exocad, 3Shape, and in-house lab software.
Upgrade Your Digital Workflow in 2026
Get full technical data sheets, compatibility reports, and OEM pricing for Scanner Cbct.
✅ Open Architecture
Or WhatsApp: +86 15951276160